Know Your Brain: Corticospinal Tract
Where is the corticospinal tract?
The corticospinal tract is a collection of axons that carry movement-related information from the cerebral cortex to the spinal cord. About half of these axons extend from neurons in the primary motor cortex, but others originate in the nonprimary motor areas of the brain as well as in regions of the parietal lobe like the somatosensory cortex. Corticospinal tract neurons project from these cortical areas down through the brainstem and into the spinal cord, where they synapse on neurons that directly control the contraction of skeletal muscle.
What is the corticospinal tract and what does it do?
The corticospinal tract is one of the major pathways for carrying movement-related information from the brain to the spinal cord. Signaling along the corticospinal tract seems to be involved in a variety of movements, including behaviors like walking and reaching, but it is especially important for fine finger movements like those that might be involved in writing, typing, or buttoning clothes. After selective damage to the corticospinal tract, patients are usually able to regain the ability to make crude movements (e.g. reaching) after a period of time, but they may be unable to fully recover the ability to make individual finger movements. This suggests other tracts are involved in most aspects of voluntary movement, and that they can generally compensate for the loss of corticospinal tract innervation; individual finger movements, however, may be a function the corticospinal tract is solely or primarily responsible for.
As mentioned above, the corticospinal tract originates in several cortical areas, with about half of the neurons that make up the tract coming from the primary motor cortex. The neurons that travel in the corticospinal tract are referred to as upper motor neurons; they synapse on neurons in the spinal cord called lower motor neurons, which make contact with skeletal muscle to cause muscle contraction.
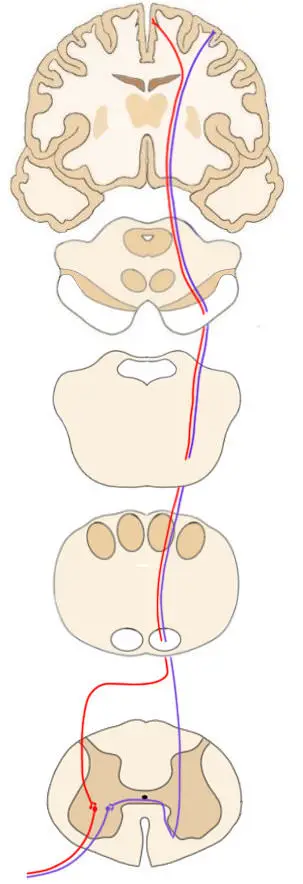
The axons that travel in the corticospinal tract descend into the brainstem as part of large fiber bundles called the cerebral peduncles. The tract continues down into the medulla where it forms two large collections of axons known as the pyramids; the pyramids create visible ridges on the exterior surface of the brainstem. At the base of the pyramids, approximately 90% of the fibers in the corticospinal tract decussate, or cross over to the other side of the brainstem, in a bundle of axons called the pyramidal decussation. The fibers that have decussated form the lateral corticospinal tract; they will enter the spinal cord---and thus cause movement---on the side of the body that is contralateral to the hemisphere of the brain in which they originated. The other 10% of the corticospinal tract fibers will not decussate; they will continue down into the ipsilateral spinal cord; this branch of the corticospinal tract is known as the anterior (or ventral) corticospinal tract. Most of the axons of the anterior corticospinal tract will decussate in the spinal cord just before they synapse with lower motor neurons. The fibers of these two different branches of the corticospinal tract preferentially stimulate activity in different types of muscles. The lateral corticospinal tract primarily controls the movement of muscles in the limbs, while the anterior corticospinal tract is involved with movement of the muscles of the trunk, neck, and shoulders.
As they travel down to the spinal cord, corticospinal tract neurons send off many collateral fibers that make connections in a number of areas including the basal ganglia, thalamus, various sensory nuclei, etc. Additionally, corticospinal tract fibers terminate in various places in the spinal cord, including the posterior horn (which is normally involved in processing sensory information). These diverse connections suggest that the functions of the corticospinal tract are likely diverse as well, and that defining it as having movement as its sole function is an oversimplification.
When the upper motor neurons of the corticospinal tract are damaged, it can lead to a collection of deficits sometimes called upper motor neuron syndrome. When such an injury occurs, it often results in a state of paralysis or severe weakness immediately following the event, usually on the side of the body opposite to the location of the injury. After several days, function begins to return, but some abnormalities persist. The patient often displays spasticity, which involves increased muscle tone and hyperactive reflexes; motor control may also be decreased. As mentioned above, after damage to the corticospinal tract the ability to make crude movements generally returns but some deficit in fine finger movements may remain. Also, patients may display other abnormal reflexes; the best known of these is the Babinski sign. When the sole of the foot is stroked it generally causes the toes in adults to curl inwards; in someone with damage to the corticospinal tract the toes fan outwards, an abnormal movement referred to as the Babinski sign after neurologist Joseph Babinski. In infants, it is normal to observe the Babinski sign due to the fact that the corticospinal tract is not yet fully myelinated. Thus, the lack of a Babinski sign in infants is considered abnormal and potentially problematic, while the presence of a Babinski sign is adults is pathological and indicates possible corticospinal tract damage.
Reference:
Nolte J. The Human Brain: An Introduction to its Functional Anatomy. 6th ed. Philadelphia, PA. Elsevier; 2009.